what to expect after Knee Replacement
Knee Replacement Surgery
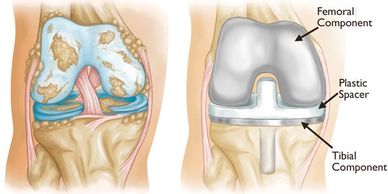
With arthritis, the weight bearing surfaces of the knee joint become worn which leads to stiffness and pain. A total knee replacement replaces these surfaces with plastic and metal. The femoral replacement is a smooth metal component, which fits snugly over the end of the bone. The tibial replacement is in two parts, a metal base sitting on the bone and a plastic insert, which sits between the metal base on the tibial and femoral component.
Knee replacement surgery usually takes about 1-2 hours.
Day of Surgery

You are usually admitted to hospital on the morning of surgery. The hospital staff at the will call to advise your admission time. You need to take relevant x-rays, current medications and their prescriptions.
On the day of surgery you will see your surgeon and anaesthetist before your operation. An anaesthetic will be administered in theatre. This may be a general anaesthetic (where you will be asleep) or a spinal block (where the area to be operated is completely numbed).
You will wake up in the recovery ward and then be transferred back to your room.
You will be encouraged to stand and take a few steps on the same day as your surgery with the use of a walking frame.
Early Recovery After Surgery
Early Recovery After Surgery

Your physiotherapist will assist you to get out of bed and walk a short distance. This will be progressed over a few days, till you are independently mobile.
You will be encouraged to get up and out of bed as much as possible, and shown exercises to improve the strength and regain the range of motion of the knee.
After a few days you should be walking reasonably comfortably for short distances, be able to manage stairs, and dress and care for yourself independently.
In the first few days avoid maintaining one position for prolonged periods. You should periodically move your knee through full range, sit out of bed, and take regular walks. We encourage you to take all of your meals sitting out of bed and dress in normal loose fitting comfortable day clothes.
Knee and Wound Care
Knee and Wound Care
Early Recovery After Surgery

Immediately after surgery some knee discomfort and swelling is normal, and is just part of the healing process. Ice packs should be used regularly to help reduce the pain and swelling in your knee. You will be given regular pain relief. The swelling causes a tight feeling in the knee which may take many weeks to months to subside.
When you leave hospital your knee wound will be covered with a waterproof dressing. This should remain in place until 2 weeks after surgery. The sutures will usually be absorbable that naturally dissolve and be absorbed by the body as a wound heals. Once the dressings are removed the wound may appear slightly red and raised with small scabs which are normal. It will slowly heal usually to a fine white scar over about a year.
Going Home
Knee and Wound Care
Ongoing exercises

Most patients stay in hospital for 3-5 days, and then go home. Wherever possible we encourage you to go home to continue your rehabilitation. Current evidence including our published research suggests that routine prolonged stay in rehabilitation hospitals is not beneficial.
The hospital staff will guide your ongoing treatment in the form of either home visits, outpatient rehabilitation classes or a self directed exercise program.
You will be provided with medications to take home to manage your pain. You should schedule an appointment with your GP for a check up within the first week of going home.
Most patients will be walking with crutches when you return home.
Ongoing exercises
Knee and Wound Care
Ongoing exercises

Once home we encourage you to perform your exercises regularly and commence a walking program.
Activity trackers such as an apple watch or fitbit can be useful to track your activity level. In general aim for 1000 steps per day in week one and increase your goal by 1000 steps each week.
Simple exercise pedals can be a useful adjunct to your exercises and can generally be purchased inexpensively. An exercise bike is also encouraged once you have achieved sufficient range of movement.
Regular application of ice packs or use of a hired commercial ice machine can be helpful in relieving discomfort.
When at rest elevating the knee is usually advisable in the first 6 weeks, but avoid maintaining any one position for prolonged periods. Regularly move your knee through full range and walk.
What to expect in the first few months
What to expect in the first few months
What to expect in the first few months

It is common to have some soreness, stiffness and swelling in your knee for about six to nine months after surgery, especially with activity.
Local numbness on the outer side of the knee wound is expected. The knee may also feel slightly warm for this period.
Pain medication are often used until about 4- 6 weeks after knee replacement but should be tailored to the individual symptoms. Narcotic medications should be ceased as soon as tolerated. After 6 weeks intermittent pain medications can be used before or after physiotherapy sessions or exercising if required.
Sleep disturbance in the first few months is common. You may sleep in any position that you find comfortable.
Walking is encouraged as exercise, and an excellent goal is about 7000 steps per day for healthy adults over 65 years.
Driving
What to expect in the first few months
What to expect in the first few months

Most people can usually return to driving after a knee replacement once they can safely control the car—particularly being able to do an emergency stop without hesitation or pain.
Right knee : Studies suggest most people regain safe braking times around 6 weeks. Because the right leg controls the accelerator and brake, you’ll generally need 6 weeks before reaction times return to safe levels.
Left knee (automatic car): You may be able to drive sooner, often at around 3 weeks, since the right leg is used for braking and accelerating.
Key factors before resuming driving:
No longer taking strong painkillers (like opioids) that impair reaction or judgment.
Able to walk comfortably and bear weight on the leg.
Good control and strength in the knee, with adequate range of motion.
Practice in a safe setting first, such as an empty car park, before going on the road.
Travel and Flying
What to expect in the first few months
Sports and Activities

It is usually safe to take a short flight a week after surgery as long as you do not have blood clots in your legs. Long flights are best avoided during the first few months after surgery, as there is a risk of deep vein thrombosis (blood clots in the legs).
If you must travel in the first few months, we recommend you wear TED stockings, mobilise throughout the flight as much and keep your legs elevated when seated during the flight if possible. If it is necessary to travel long distances, then speak to your GP or surgeon prior to doing so. They may also recommend you take some preventative medications.
You should not plan significant travel which would involve a lot of daily walking for at least 3-6 months after knee replacement surgery.
Sports and Activities
Sports and Activities
Sports and Activities

Swimming, golf, walking, cycling, lawn bowls, gardening and social tennis are examples of excellent options to explore to keep fit after knee replacement. However, you should plan to refrain from exercises such as pilates, golf and social tennis until about 2-3 months after surgery.
With all sporting activities, it is best to gradually increase intensity in line with how your knee feels.
Golf: Start by practicing at the driving range or putting green, and consider using a cart at first.
Tennis: Begin by hitting gently with a friend, and try doubles before progressing to singles.
Cycling: Start on a stationary bike before moving to outdoor cycling.
High-impact sports involving jumping, running, and quick pivoting, such as basketball and football, should generally be avoided.
If you are enthusiastic about a particular sport, please seek instructions from your surgeon.
Kneeling
Sports and Activities
Dental Procedures

There is no evidence that kneeling on a knee replacement damages the prosthesis, though numbness around the scar is common and can make kneeling uncomfortable.
Desensitization—gently practicing kneeling on soft surfaces and gradually progressing to firmer ones —helps your knee adjust to the altered sensation and reduces discomfort over time. This can be started from 6 weeks after surgery.
Always check the surface with your hand before kneeling, and consider using knee pads for activities like gardening.
Dental Procedures
Sports and Activities
Dental Procedures

After joint replacement current evidence suggests that routine use of antibiotics for all dental procedures is not indicated. Rather this decision should be based on the expected associated risk of infection associated with the procedure. For routine non surgical dental treatments, including extractions no antibiotics are required, unless
otherwise indicated.
Prophylactic antibiotics may still be considered for patients with high risk such as
- Immunocompromised status: Patients with weakened immune systems are at a higher risk.
- Recent surgery: A dental procedure within the first three months after a joint replacement is a higher-risk situation.
- Infection from a dental problem: Dental treatments for established tooth infections are more likely to require antibiotics.
Preparing for Knee Replacement
Preadmission Appointments
Preparing for Surgery with Diet
Preadmission Appointments

You should arrange to attend the Mater Hospital preadmission clinic before surgery to be meet with an Anesthetist and hospital staff. If you live remotely this can be organised over the telephone. You can discuss your medical history and options for your anaesthetic. This should be scheduled for 2-4 weeks prior to your surgery. Phone: (02) 9900 7494
Prior to you appointment complete the online admission and registration form, and have your pre-operative blood tests. If your Surgeon has asked for a review with a cardiologist or Physician, have this prior to your Pre-Admission appointment.
You should also contact the Mater Continuous Care Team who can assist in your preparation for surgery and discharge to home.
Managing Medications
Preparing for Surgery with Diet
Preadmission Appointments
You should disclose to your anaesthetist if you are taking any blood thinners, hormone tablets, diabetes or weight loss medications. Your anaesthetist will give you individual advice, but in general you should stop arthritis medications such as anti-inflammatories for one week prior to surgery as they increase bleeding. Take only panadeine or paracetamol for pain relief during this period. GLP-1 receptor agonists (such as semaglutide [Ozempic, Wegovy], dulaglutide [Trulicity], liraglutide [Saxenda/Victoza]) Tirzepatide (Mounjaro®) are being used more widely for both diabetes and weight management. GLP-1 medications slow down stomach emptying. This can increase the risk of vomiting or aspiration (food or fluid going into the lungs) during anaesthesia. To keep you safe, these medicines are usually paused a few weeks before surgery. Your anesthetist will give you specific instructions for your individual case.
Preparing for Surgery with Diet
Preparing for Surgery with Diet
Preparing for Surgery with Diet
Eating well rounded meals in the weeks before surgery emphasizing complex carbohydrates and especially high quality proteins which will support recovery and strength. Protein intakes of 1.2-2.0g/kg/day is recommended in the weeks before surgery. Supplements can be helpful in achieving these goals. If you have diabetes, it is important to keep blood sugar under good control — this lowers risk of infection and helps healing.
Alcohol increases bleeding risk and may interact with anaesthetic so is best avoided in the week before surgery. High-salt foods may increase swelling and blood pressure.
Eat a balanced meal the night before: lean protein, vegetables, and whole grains, and avoid alcohol and heavy, fatty, or spicy meals that can upset your stomach.
You will usually be asked to fast from midnight the day before surgery which means you should have no food, and drink clear fluids only.
Preparing your home
Strength and Exercises
Preparing for Surgery with Diet
Make Moving Around Safer
Clear walkways: remove loose rugs, cords, and clutter to prevent tripping. Ensure hallways, stairs, and bathrooms are well lit. Check that any stair rails and grab bars are secure.
Set Up Comfortable Living Spaces
Make sure you have a firm, supportive chair with arms that is not too low, to make standing up easier. If your bedroom is upstairs, consider setting up a temporary sleeping space downstairs until you are comfortable. However you will be instructed on safe stair climbing before you go home, so stairs will be manageable.
Plan for Meals & Essentials
Stock up on groceries: freeze easy meals or prepare healthy options ahead of time.
Keep essentials handy: place frequently used items (phone, TV remote, medications, water bottle) within easy reach at waist level.
In the kitchen move frequently used items out of low or high cupboards so they can be easily accessed.
Consider help: arrange for family, friends, or community services to assist with shopping, cooking, or cleaning in the first few weeks.
Mobility & Equipment
Strength and Exercises
Strength and Exercises
Ensure you have supportive and comfortable shoes, with a flat grip sole that fully enclose your feet
Walking aids: you will likely use crutches or a stick when you return home. These can be purchased or hired before surgery. Before surgery, practice and get comfortable using these aids around your home.
Bathroom aids: a raised toilet seat, shower chair, and non-slip mats can make bathing safer.
Pet care: make arrangements if you have pets that may get underfoot or need walking.
Transport: arrange who will drive you home from hospital and to follow-up appointments (you won’t be able to drive for several weeks).
Strength and Exercises
Strength and Exercises
Strength and Exercises
Some simple exercises can be beneficial in improving the strength of your knee before surgery, which may assist your post operative recovery.
Use of a stationary exercise bike is encouraged.
Some other simple exercises such as wall squats, and gluteal bridges are shown above.
You may benefit from an appointment with a physiotherapist if you would like a more personalized program.
Walking is encouraged as exercise, and an excellent goal is about 7000 steps per day for healthy adults over 65 years.
This video available on the Mater Hospital website may also be a useful guide.
Long term outcomes of knee replacement
NSORG Outcomes of Knee Replacement

Since 2015, the surgeons of the North Sydney Orthopaedic Research Group have followed more than 10,000 patients before and after hip and knee replacement surgery. We collect information at before surgery, 6 months, and 12 months after surgery to understand recovery and outcomes.
Satisfaction With Knee Replacement
- 91% of patients said they were satisfied or very satisfied with their knee replacement at 12 months.
- 87% said they would choose to have the same operation again under the same circumstances.
Pain Relief
- Before surgery, only 11% of patients reported no or only mild pain when walking.
- By 6 months after surgery, this increased to 93%.
- By 12 months, 96% of patients reported no or only mild pain.
Activity Levels
In a smaller study of 160 patients who wore a wrist-worn step counter:
- At 6 months, patients walked 130% more steps each day compared to before surgery.
- 70% were more active than they were before their operation.
Sleep
In our published study of 780 patients:
- 35% reported poor sleep quality before surgery. This was more common in women
- After surgery, 74% of those with poor sleep improved quality
- Before surgery, 42% patients reported less than 6 hours of sleep. After surgery, 67% of reported an increase in sleep duration after surgery.
Depression and Anxiety
In our study of 3,232 knee replacement patients:
- Half reported some level of depression or anxiety before surgery.
- Moderate to severe depression or anxiety dropped from 21% before surgery to 8% after surgery.
- Of those with moderate to severe symptoms before surgery, 75% improved within 12 months.
- Patients with depression or anxiety tended to start with lower scores, but improved just as much (or more) than other patients after surgery.
Take-home message:
Most people experience substantial pain relief, high satisfaction, better activity levels, and improved sleep and mood within the first year after knee replacement surgery with surgeons from North Sydney Orthopaedic Research Group.
Outcomes from Australian Joint Registry

The Australian Orthopaedic Association National Joint Registry (AOANJRR) tracks every knee replacement that is performed in Australia for further surgery that is required. There were 1,026,935 knee replacements reported to the Registry as at 2025.
The AOANJRR tracks "revision surgery" — meaning removal, replacement, or addition of any device component. After knee replacement the percentage of patients that have not had any revision surgery is 97% at 5 years, 95% at 10 years and 94% at 15 years and 92% at 20 years. This bodes well for the long term survival of modern knee replacements.
Age has been identified as the most important patient factor that influences the risk of revision. The younger the patient, the higher the risk of revision.
Knee replacement surgeries in Australia generally have excellent outcomes. Most patients report substantial improvements in pain, function, and overall quality of life—a finding supported by real-world data covering nearly all knee replacements in the country. The rates of needing further surgery (revision) are low, and have improved over time thanks to better implants and refined surgical methods.